


Background: Classical Hodgkin lymphoma (CHL) patients (pts) requiring second line therapy may still be cured with multiagent salvage chemotherapy followed by autologous stem cell transplant (ASCT). The likelihood of long-term remission following ASCT for relapsed/refractory (R/R) CHL is predicted by response to pre-ASCT salvage therapy (Moskowitz et al. Blood 2012). The anti-CD30 antibody-drug conjugate brentuximab vedotin (BV) is effective as a single agent in R/R CHL. We hypothesized that concurrent therapy with dose-dense BV and 2 cycles of ICE would be safe, efficient, and produce high CR rates necessary for superior outcomes after ASCT. (#NCT02227199)
Methods:
Patients (pts) ≥ 18 years old with first relapse or primary refractory CD30+ cHL were eligible for this IRB-approved prospective clinical trial. Treatment included BV on Days 1 and 8 at either 1.2 or 1.5 mg/kg (based on 3+3 dose-escalation schema; capped at 150 mg), ifosfamide and mesna 5 g/m2 each on Day 2, carboplatin AUC 5 (capped at 800 mg) on Day 2, and etoposide 100 mg/m2 daily on Days 1-3. Two 21-day cycles were given with G-CSF support. BV 1.5 mg/kg was selected as the phase II dose based on reported dose escalation data (ASH 2016, #1834). PET was performed after Cycle 2, with response assigned per Cheson 2007. Stem cells were collected after Cycle 2 at discretion of treating investigator. Peripheral blood (PB) pre- and post-treatment, stem cell (PBSC) product, and (when available) archived formalin-fixed paraffin-embedded tissue (FFPET) from presentation and relapse were collected for correlative studies. Pre-treatment PB cytokine levels were measured by Luminex. Immunohistochemistry (IHC) on FFPET identified components of inflammatory microenvironment.
The primary endpoint was to determine the MTD and CR rate after 2 cycles. Secondary endpoints included PFS, OS, stem cell collection, and molecular correlates.
Results: All 45 pts have enrolled and completed study treatment, including 42 pts who were assigned treatment at the MTD of 1.5 mg/kg on day 1 and 8 of each cycle. Median age was 31 (range, 21-61). 16/45 (36%) were male, 28/45 (62%) had primary refractory disease, and 11/45 (24%) had extranodal involvement at relapse.
41 pts completed both cycles of therapy. One pt experienced grade 5 multi-system organ-failure during cycle 1, one pt was removed from protocol due to non-compliance, and two pts omitted cycle 2 due to toxicity (grade 4 sepsis, grade 3 Sweet syndrome attributable to G-CSF). 2 pts received all ICE dosing, but omitted at least one dose of BV due to toxicity. In addition, 13/41 (32%) pts delayed initiation of cycle 2 by a median of 7 days (range 6-17) due to toxicity, primarily elevated transaminases (10/13, 77%). 16/45 (36%) pts experienced neuropathy, but grade ≥2 neuropathy was rare (3/45, 7%). Other grade 3-4 non-hematologic toxicity included febrile neutropenia/sepsis (11%), elevated ALT (11%), hyperglycemia (7%), pulmonary embolism (4%), and elevated AST (4%).
36 pts underwent PBSC collection at our institution and had all data available for analysis. 30/36 pts were able to collect at least 5x106 CD34+ cells/kg. 5/6 of the remaining pts were still able to proceed with ASCT with the amount collected, and the other pt was not deemed an ASCT candidate due to social reasons. 37/43 pts (86%) who were evaluable for response proceeded to ASCT (2 subjects declined ASCT, 2 were ineligible due to social issues, one was lost to follow up, one remained chemorefractory despite additional salvage chemotherapy). Only 4/37 pts who received an ASCT subsequently relapsed.
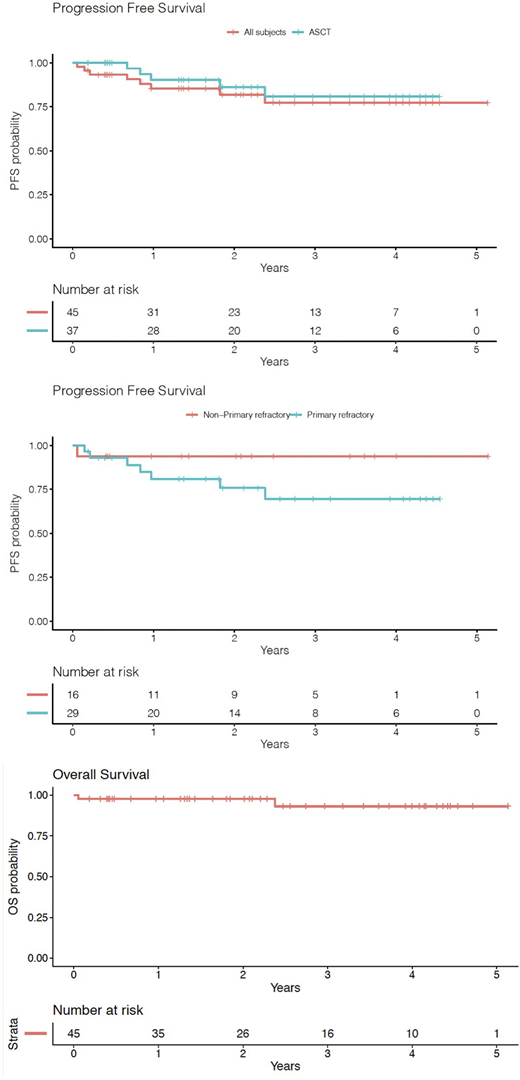
43 pts were evaluable for efficacy. Overall response rate (ORR) and CR for all enrolled patients were 91% and 74%, respectively. Among primary refractory pts, ORR and CR were 86% and 68%, respectively.
With a median follow-up of 26.5 months (range 0.7-62) months, 2-year PFS and OS were 82% and 98%. Updated results will be presented at the meeting.
Conclusions: BV-ICE is a rapid, active and tolerable salvage regimen for R/R CHL patients, including those with primary refractory disease. Efficacy results are comparable to previously presented BV-chemo salvage combinations often delivered over longer durations. BV-ICE should be considered in R/R CHL prior to ASCT.
Lynch:Juno Therpeutics: Research Funding; TG Therapeutics: Research Funding; Takeda: Research Funding; Incyte: Research Funding; Rhizen Pharmaceuticals: Research Funding; Bayer: Research Funding; Cyteir: Research Funding; MorphoSys: Consultancy; Genentech: Research Funding. Cassaday:Merck: Research Funding; Amgen: Consultancy, Research Funding; Pfizer: Honoraria, Research Funding; Vanda Pharmaceuticals: Research Funding; Seattle Genetics: Current Employment, Current equity holder in publicly-traded company; Kite/Gilead: Consultancy, Research Funding. Smith:AstraZeneca: Research Funding; Acerta Pharma BV: Research Funding; Beigene: Consultancy; Millenium/Takeda: Consultancy; AstraZeneca: Consultancy; Seattle Genetics: Research Funding; Portola: Research Funding; Pharmacyclics: Research Funding; Merck: Research Funding; Incyte: Research Funding; Ignyta: Research Funding; Genentech: Research Funding; De Novo Biopharma: Research Funding; Bristol Meyers Squibb: Research Funding; Bayer: Research Funding; Ayala: Research Funding; Karyopharm: Consultancy. Fromm:Merck: Research Funding. Cowan:Abbvie: Research Funding; Bristol Myers Squibb: Research Funding; Cellectar: Consultancy; Sanofi: Consultancy; Janssen: Consultancy, Research Funding. Shadman:Mustang Bio, Celgene, Pharmacyclics, Gilead, Genentech, Abbvie, TG therapeutics, Beigene, Astra Zeneca, Sunesis, Beigene: Research Funding; Abbvie, Genentech, Astra Zeneca, Sound Biologics , Pharmacyclics, Verastem, ADC therapeutics, Beigene, Cellectar, BMS, Morphosys and Atara Biotherapeutics: Consultancy. Shustov:Seattle Genetics: Research Funding. Till:Mustang: Patents & Royalties, Research Funding. Ujjani:MorphoSys: Consultancy; Genentech: Consultancy, Honoraria; Atara: Consultancy, Honoraria; Gilead/Kite: Consultancy, Research Funding; Verastem Oncology: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria, Research Funding. Gopal:IgM bio, BMS, merck: Research Funding; imab bio, takeda,astrazeneca,gilead: Research Funding; Seattle Genetics; Janssen; Takeda; IgM Bio; IMab Bio; BMS; Astra Zeneca; Merck; Gilead: Research Funding; Seattle Genetics; Janssen; IMab Bio; TG Therapeutics; Astra Zeneca; Merck; Gilead; ADC Therapeutics; Nurix; TG therapeutics, Cellectar; Actinium: Consultancy.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal